Ventilators are a key treatment for Covid-19, and there has been a wave of interest concerning development of low-cost ventilators; especially with a projected Covid-19 wave in excess of 100 millions for Africa. Here, then, is the Israel developed AmboVent, one of something like 300 fast-track initiatives to develop such globally:

This is of course one of several designs pivoting on the nearly ubiquitous manual respirator bulb, as per a suggestion that has been on the table for some time. Now we see a [near-?] commercial product. Video on the suggestion:
Their blurb:
The AmboVent initiative is led, by the Israeli Air Force (IAF) 108 electronic depot in partnership with Magen David Adom (MDA) (Israel’s red cross). The R&D phase was backed by a large community of innovators, to include: makers from First Robotics Israel (mentors and students), physicians from leading Israeli hospitals such as Tel Aviv Sourasky and Hadassah JLM as well as other medical centers, Engineers from Haifa Technological Center and The garage program by Microsoft Israel, IAF Unit 108, and more. All have joined the endeavor on a voluntary basis. This Ad hoc team work together as an open organization aiming at providing in an ultra-short time a viable, usable, simple and intuitive to use mechanical ventilator.
This is obviously globally deployable and could readily be set up in even an Ambulance. As a news article suggests:
“This can ventilate millions in Africa when no other machine is around,” Eliram was quoted by the Times of Israel as saying. “In Africa, they haven’t fully woken up to the coronavirus and there are hardly any ventilators, so this can make a huge difference.”
World Health Organization statistics show that there are only 2,000 ventilators in the whole of Africa – less than the amount in Israel. Some African countries don’t have any. A report by the UN Economic Commission for Africa said the continent, which is a few weeks behind Europe in regards to the spread of the pandemic, will likely be dealing with 122 million infections.
AmboVent is also producing 20 prototypes to send to other countries on a limited budget of $200,000. The team is also launching a crowdfunding campaign.
“The situation with ventilators is dire,” Eliram said. “Even with some of the ventilators you can get, you can’t get the valves anymore, so people are calling and saying we want this machine that isn’t dependent on sourcing supplies after it is made.”
AmboVent uses a robotic arm to operate a bag-valve mask, like the kind used in ambulances, the connects to the patient through an intubation tube.
“It’s a second-choice compassion device,” Eliram said. “This is your plan B in the hospital, once you’ve exhausted all your $40,000 machines.”
Of course, one is tempted to ask as to whether there will be a demand for double-blind, placebo control group testing to “prove” the efficacy of such a device before it should be deployed.
To which the obvious answer is, no. No, as it would be unethical to treat someone dependent on artificial respiration with a deliberately ineffective treatment (apart from “belief kills and belief cures”). No, because the obvious near- Business as Usual baseline is a very tight stock of US$ 40 – 50,000 ventilators and/or to deploy a huge proportion of skilled staff to manually pump ventilators on a 24/7 basis (manually pumped Ambu-Bags are designed for short term emergency or bridging use), when they could be better deployed to other urgently needed tasks. No, because we can trace the dynamics at work and can see the rationale’s soundness.
In short, the Gold Standard fallacy is exposed yet again.
There is no one size fits all cases and circumstances Gold Standard way to validate innovative treatments.
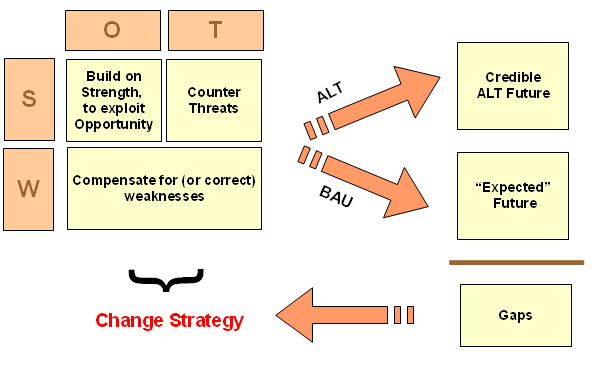
What is arguably a more valid approach is to extend a SWOT-driven, sustainable development strategic decision model to the context of deciding whether a medical treatment innovation credibly offers an improvement over the BAU-baseline expected future, then using this to drive a robust strategic change process. As I have illustrated:
I trust this note will be helpful.
Let’s trust that this and similar devices can reach Africa in good time, with the sort of magnitude of Covid wave being feared. END
PS: This video is very similar to the recent one on using UV to kill pathogens in breathing passages; it even extends to the similar context of assisted breathing. Is YT going to “kill” this one too for violating its [nebulous?] “standards”?