There is a report that Azithromycin is far more than an antibiotic. Some may wish to watch an interview with Dr. Michael Lisanti on antibiotics for COVID-19 and cancer. But — without endorsing as “proved” fact — let’s cut to the chase scene:
COVID-19 coronavirus is particularly dangerous for the elderly or those with aging-related senescent illnesses like diabetes, cancer, heart disease, and lung disease. As Professor Lisanti said in a statement on his new paper in the journal Aging, “If you look at the host receptors of COVID-19, they are related to senescence. Two proteins have been proposed to be the cellular receptors of COVID-19: one is CD26 – a marker of senescence, and the other, ACE-2, is also associated with senescence. So, older people would be predicted to be more susceptible to COVID-19, exactly as is observed clinically in patients. This could increase their probability of infection, and would explain the increased fatality of COVID-19 infection in older patients. All of this could be related to advanced chronological age and senescent cells.”
Lisanti’s laboratory has previously demonstrated that Z-pak [a version of Azithromycin] selectively removes 97% of senescent cells. Without those cells acting as host receptors, it may be harder for COVID-19 to take root in the body and cause serious damage.
Lisanti’s lab goes on, “Clinically, it appears what is leading to fatalities in older [COVID-19] patients is the very strong inflammatory reaction and the resulting fibrosis. Azithromycin inhibits inflammation-induced fibrosis, by targeting and removing senescent cells. The cost would be minimal, as the drug is off-patent, widely available and considered safe.”
Z-pak has made headlines after doctors around the world such as the widely publicized French clinic trials and New York and New Jersey physicians have found promising results on the front-lines of coronavirus using it in combination with another generic drug hydroxychloroquine . . . .
But, but, but, doesn’t an antibiotic work against Bacteria? Yes, the issue is HOW, and whether the cluster of effects of a given drug may also be effective against the viral replication-by-hijacking cycle.
A hypothesis is posed:
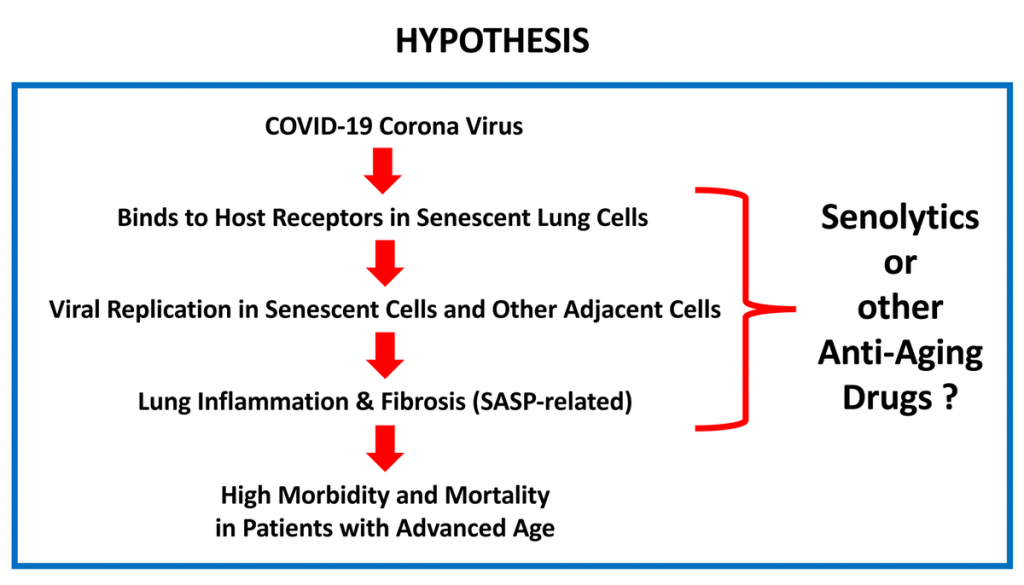
In the paper, we also find:
Recently, a clinical trial was conducted using COVID-19 positive hospitalized patients, which assessed COVID-19 virus production in response to treatment with two FDA-approved drugs, namely Hydroxy-chloroquine (Plaquenil) and Azithromycin (Z-PAC) [13]. Hydroxy-chloroquine alone, at the standard dosages, was surprisingly effective in reducing COVID-19 viral production. However, the combination of Hydroxy-chloroquine and Azithromycin appeared to be even more effective. The mechanism(s) by which this drug combination halts COVID-19 virus production remains unknown . . . . Chloroquine and its derivatives, such as Hydroxy-chloroquine, alkalinize the pH in lysosomes, which accumulate in large numbers in senescent cells. This Chloroquine-induced alkalinization functionally prevents the induction and accumulation of one of the most widely-recognized markers of senescence, known as beta-galactosidase (Beta-Gal), a lysosomal enzyme [14]. Hydroxy-chloroquine is also used clinically for the treatment of chronic inflammatory diseases, such as Sjögren’s syndrome, and it effectively reduces the salivary and serum levels of IL-6, a key component of the SASP [15].
This of course is a suggested mechanism that may well be working in parallel with the Zn ionophore effect.
That rather reminds me of the Allied shock of finding the Germans using an anti-aircraft gun in the anti-tank and bunker-busting role, the infamous 88-mm gun originally developed by the Krupp concern. Soon it had mutated into a whole family of guns, especially in the notorious Tiger tank family. By contrast, it was after the war that the British were able to fully develop the 20 pounder, which IIRC, was at least influenced by the UK 3.7 inch AA gun, which was far heavier than the German 88. (Mind you, in North Africa, they diverted the 25 pounder Gun-Howitzer to the antitank role, a calibre 87.6 mm weapon derived from the earlier 18 pounder and also replacing the 4.5 inch howitzer as a standard field gun.)
In short, flexibility is a relevant and potentially decisive matter.
The same article puts some further food for thought on the table:
New drugs cost a billion dollars and 10-15 years to make it through the FDA approval process. This regulatory hurdle precludes natural substances that cannot be patented from being properly researched and tested for illnesses because companies cannot afford the cost to prove the efficacy of something that any organization would be able to sell afterwards. This top-down monopoly approach to medicine can leave the world on its heels—not enough clinical trials on natural substances and patent-dependent, new FDA-d drugs and vaccines years away—during a pandemic like the one we are in now.
Some, would suggest, that’s not a bug, it’s a feature.
We need to be asking some very pointed questions about drug development, trials and strategies for an emerging age of pandemics. END