It is clear that we need to re-think how we go about doing science to warrant approaches to the pandemic. So, allow me to headline a comment from the double-blind thread:
KF, 16: >> I am also thinking back to the old “Scientific Method” summary we were taught in schools and its roots in Newton’s Opticks, Query 31:
As in Mathematicks, so in Natural Philosophy, the Investigation of difficult Things by the Method of Analysis, ought ever to precede the Method of Composition. This Analysis consists in making Experiments and Observations, and in drawing general Conclusions from them by Induction, and admitting of no Objections against the Conclusions, but such as are taken from Experiments, or other certain Truths. For [speculative, empirically ungrounded] Hypotheses are not to be regarded in experimental Philosophy. And although the arguing from Experiments and Observations by Induction be no Demonstration of general Conclusions; yet it is the best way of arguing which the Nature of Things admits of, and may be looked upon as so much the stronger, by how much the Induction is more general. And if no Exception occur from Phaenomena, the Conclusion may be pronounced generally. But if at any time afterwards any Exception shall occur from Experiments, it may then begin to be pronounced with such Exceptions as occur. [–> this for instance speaks to how Newtonian Dynamics works well for the large, slow moving bodies case, but is now limited by relativity and quantum findings] By this way of Analysis we may proceed from Compounds to Ingredients, and from Motions to the Forces producing them; and in general, from Effects to their Causes, and from particular Causes to more general ones, till the Argument end in the most general. This is the Method of Analysis: And the Synthesis consists in assuming the Causes discover’d, and establish’d as Principles, and by them explaining the Phaenomena proceeding from them, and proving [= testing, the older sense of “prove” . . . i.e. he anticipates Lakatos on progressive vs degenerative research programmes and the pivotal importance of predictive success of the dynamic models in our theories in establishing empirical reliability, thus trustworthiness and utility] the Explanations. [Newton in Opticks, 1704, Query 31, emphases and notes added]
Now, obviously, case-based, reliability driven, insightful inference to best current explanation oriented inductive investigations and reasoning are much broader than the conventionally labelled sciences. That’s a piece of why there is no one size fits all and only Big-S “Science” method. But it is undeniably powerful and when properly done, useful.
My favoured summary (honouring a favourite student) is O, HI PET:
O — OBSERVE a situation (looking at key factors, facts, trends, relationships, family resemblances etc, the intent being to accurately describe, effectively and reliably explain, reliably predict patterns, and use these to influence or control fresh situations)
H –HYPOTHESISE . . . infer an evident pattern (looking for reliable, best current explanatory frameworks)
I & P — INFER & PREDICT . . . what consequences would follow in fresh circumstances (an empirically reliable principle, rule, explanatory framework, law, model or theory — or entity embedding such — is highly valuable . . . including a new instrument, device, gadget, process, procedure or treatment embedding such)
ET — EMPIRICAL TESTING . . . we need to identify then disseminate successful, reliable, effective, insightful, fruitful results
Now, let’s state the needed obvious: nothing in this framework mandates double-blind, placebo control group procedure.
Indeed, it points to the underlying principle of case-based reliable inference. Where control groups can ethically and effectively be deliberately set up and used, fine. But that is by no means always the case, with Astronomy perhaps the capital example as a sub-discipline that uses case-based observational studies as a part of the hardest of the hard sciences, Physics. There is a reason why we speak of Astronomical OBSERV-atories, not LABOR-atories. (Ditto for Volcanology; and that was the pivot of my public warning here, 25 years ago. Looong story.)
In short, we must be humble enough to recognise that we cannot prescribe an investigative panacea.
Linked, we may ask, how does this work?
First, by applying the principle of distinct identity. A is A i/l/o its key characteristics, some in common with near and increasingly distant neighbours, some more specific to its class then ultimately to itself as a particular case. Where, core characteristics give rise to repeatable patterns of behaviour in sufficiently similar situations.
Thus, the art of scientific and broader empirical investigations is to seek sufficiently reliable candidate characteristics- in- common for a broad enough class of cases or entities. This then can be tested for reliability through further studies, whether experimental, observational, predictive or “retrodictive” etc. Such, can then be accepted as a provisional, promising explanatory model, which at the high end will be a theory [i.e. an explanatory model that is felt to be possibly true; models may be deliberately simplified . . . so necessarily false, but useful].
Again, nothing in this imposes placebo control groups as a necessary criterion of validity or reliability. And, contrasted cases studied in matched pairs or clusters with variances points to a broad framework for statistical studies, ANOVA and its various extensions.
But even that is not a straightjacket, various forms of exploratory data analysis and scientific visualisation have often been powerful. Modelling- and- simulation exercises (often with computer animations and Monte Carlo explorations of contingencies) have joined such in recent years. Taxonomical studies have been fruitful, e.g. in Biology. So can be simple tabulation, with the periodic table being perhaps the classic case in point. That brings up, familiarity with epochal cases, the paradigms that set up new schools of thought and launch research programmes.
But, such programmes are almost never “proved” — in Lakatos’ terms, they are born, live and die “refuted” by anomalies, counter-examples, challenges, exceptions, open questions etc. But a progressive research programme advances through successive predictive success, and a regressive one falters and wanders off into becoming increasingly ad hoc and/or simplistic and restricted. If institutionalised in power centres, a degenerative programme can stave off competitors for many years, but eventually, the bills come due with nothing to cover them.
All of this sounds rather political and ideological, doubtless. (Economics is perhaps the capital example.)
Yes.
We are social creatures and power- with- linked- wealth is always a consideration. Which is why issues of corruption are always lurking as a dirty secret in Science; including, on what may go on behind the scenes of peer review. Likewise, we see the challenge . . . or, is that now, crisis? . . . of testing and reliable replicability.
Coming back to our immediate focus, it is obvious that urgency here undermines the relevance of placebo controlled studies, even were one to set aside the issue that first the physician must do no harm. Where, sugar pills deliberately administered to patients facing a fast acting, potentially deadly disease pose fairly obvious ethical challenges. So, we need to go to deeper investigatory principles, to identify what is a more relevant approach to a pandemic in progress.
The answer comes back, repeated, case based clinical studies using suitable candidates reflecting the state of our knowledge. Which is precisely what Prof Raoult has been doing. 2759 cases reflects Stalin’s principle: sufficiently massive quantity has a quality all of its own.*
KF
*PS: That’s so here because in this context, beyond a certain mass of cases that sufficiently contrast with the general background, errors of coincidence are not a credible candidate null explanation. If there is a 10 percent chance of error, and, we see 100 independent cases that trend is unlikely to be chance. The chance that a string of errors that long falls exponentially. 0.1^100 is 10^-100. If the die keeps coming up sixes 100 times, or the coin comes up H 100 times in a row, loading becomes the best explanation. Which is of course the basic point in classic hypothesis testing in statistics. >>
Such gains further strength in light of a further comment in the Remdesivir thread, in response to BO’H and Jerry; which I now augment as OP’s allow insertion of images:
BO’H, 3: >> Be careful – by the sounds of it, this [leak on a Chicago study on Remdesivir] doesn’t have a control group either. Hopefully some of the other trials have control groups. >>
KF, 4: >> you need to ask yourself why there is a case based rather than placebo based design, and why gold standard dismissive rhetoric fails ethically and epistemologically. >>
Jerry, 5: >> There is a control group of several thousand dead people from the virus. They got the placebo. >>
KF, 6: >>Jerry,
you are quite correct, and your remarks point to decision theory and sustainability strategies.
There is a de facto standard set of treatments tied to blocks of patients, with associated tracking results and outcomes. That is standard process, to the point that a fever chart on a clipboard attached to a bed is a stock cartoon gag. This forms the baseline and de facto benchmark or yardstick. Once one introduces an alternative, it is possible to similarly track performance then key to known demographics, once one has enough cases to reasonably span the demographics of sex, age, preconditions etc.
Though, obviously the novel treatment should have a priori credibility that points to a reasonable prospect of success that makes it worth taking the human life and health risk of trying it, as well as implied financial and resource commitment costs. For instance, in vitro studies show chemical plausibility and as there are often relevant physiological similarities, animal analogues may be relevant.
(BINGO: The lab(s) in Wuhan were apparently using bats as animal analogues, likely in studying corona virus treatments in the aftermath of SARS, MERS etc. We know HCQ etc were on the table since SARS. So, they may well have had background, classified knowledge on its potential that added reason to the explanation, it works on inflammation responses out of control. Remember, that is indeed a known complication leading to potentially deadly cytokine storm, which especially affects the elderly. Where, too, associated secondary bacterial infections can be a contributory factor. So, if a bat corona virus, under drugs pressure, mutates and bridges to humans then leaks into the population, we could project a pandemic possibility. That raises questions of behind the scenes batteries of tissue cultures and testing cultures of drugs and cocktails. Penicillin was discovered because a mould contaminated bacterial cultures and hindered growth in a ring. Currently, multidrug resistant bacterial strains are so common that it is a standard test to swab and culture vs an array of drug possibilities. This is leading to a tendency to prescribe double antibiotic cocktails that seem to be synergistic. Certainly, that is my experience. Indeed, there are strains that are now disinfectant resistant. No wonder soap and water, alcohols, vinegar as well as bleach are back as seriously considered sanitisers and disinfectants. At this point, I infer, the Chinese knew from their level 4 lab, that HCQ was a plausible candidate for not only anti-inflammatory but anti-viral action in vitro AND in animal analogue. Of course, explaining containment failure would be a truth/state secret/ losing face challenge.)
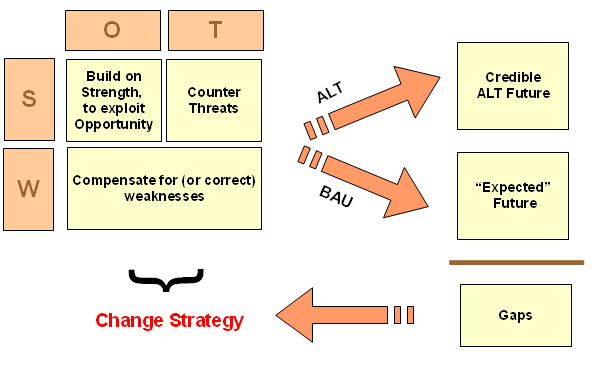
Now, let us say we have some reason for credibility, for an alternative. This then brings up a strategic decision making, sustainability frame based on SWOT, scenario projections across world models, use of proxies or known direct metrics, and the sustainability options: Business as Usual vs Credible Alternative[s]. [I insert, an image:]
The issue is to consider strategic alternatives informed by empirical evidence and scenario based broad spectrum models. Such models here obviously have to consider epidemiological, economic, sociocultural, political, legal and media factors, trends and issues as well as Game Theory extensions to simultaneously playing against nature and human players. Where, statistical aspects come from Monte Carlo scattershot runs, to see a plausible — notice, not probability distribution — pattern of possibilities, risks, opportunities, uncertainties.
On situation analysis, we get an environment threat and opportunity profile, ETOP. We extend this to strengths and weaknesses profiling. A robustly sustainable strategy fits a SWOT matrix:
* build on strengths,
* counter threats [here, natural and human in a highly polarised environment],
* exploit opportunities [here, potential new treatments involving further research],
* compensate for and where possible/ advantageous, correct weaknesses [here, need for effective broad spectrum antivirals and need to correct
faulty, cumbersome drug development protocols in a world of pandemics]
To do so, one must project across integrated world models, the spectrum of plausible outcomes on BAU trends. Which leads to the cluster of expected futures. Expected, as BAU is the result of the balance of power across factions that dominate in a situation. (This is also where the Seven Mountains picture is a handy way to discuss and explain.)
[I add, for existential, crisis situations:]
[Then, there is the old lemmings story — let’s connect a few dots:]
We then run plausible alternatives similarly, at first as games or scenario exercises, then pick best options and do additional research. From this, we have credible alternatives and may have plausibly feasible and more desirable futures. That can be identified through comparison, i.e. gap analysis.
When that is identified, we may then proceed to creating change strategies to migrate to more desirable, robust, sustainable alternatives. That is, we have a framework for a change strategy, which normally implies conflict with not just nature but entrenched power factions wedded to BAU.
It should be obvious, that at least elements of this framework are in play and help us “read” the situation, explaining a lot of what is playing out.
Now, this brings us back to the factor that conventional placebo control studies building on in vitro and animal analogue studies are first going to take too long in the face of a fast-moving pandemic. Similarly, there are vested interests and unwelcome truths are liable to be suppressed; so, we have to be discerning and prudent. Thirdly, we have an ethical-epistemological challenge that is an embedded part of an institutionalised problematique tied to entrenched BAU, as BAU will not only take too long but pivots bon deception and on mistreating patients dealing with/facing a fast-moving, deadly epidemic. This is not a slow moving cancer where we may try A, then B then C etc.
In that context the strategic change framework rationalises a case based approach. And that is precisely what Raoult et al seem to have been doing. Further, the spotlight is put on animal analogue studies. Given the significance of bats here, why is this side of the issue missing in action, especially as the ethical issues are much less intense? I suspect, this reflects factional interests and political calculation; including by the usual media suspects. Material truth is the first casualty in a war.
We can draw some conclusions:
First, that there is a reasonable, responsible framework in which a Case based approach is reasonable and epistemically plausible.
Second, that relevant powers and their spokesmen must be aware of that, so rhetoric about no evidence and gold standard testing is unethical, indeed deceitful.
Third, that media amplifiers of agit prop lines like this [Guardian, I am looking at you] are irresponsible in the face of a serious global threat, but are obviously effective in promoting BAU and the agendas of its backers.
Fourth, in the face of a global crisis, that BAU is not in the general interest of the publics in the USA, UK, France, China and beyond across the world.
Fifth, that a credible cluster of potential alternatives is on the table, warranting the pursuit of SWOT-Scenario exploration, BAU vs ALT gap analysis then creation of a change strategy to more robustly sustainable strategies with sounder governance.
Sixth, that a struggle to do so is in progress, with S Korea, France, Britain and the US as key theatres of operation.
Seventh, that we need to rethink how we consume media offerings and how we have been led to think about even statistics etc.
So, now, let us think afresh.>>
In short, no, we are not locked up to human patient, placebo control testing as a gold standard, implying that in the face of a fast moving deadly pandemic, we can only hope for credible treatments a year from now. END