And, why is that (which was announced yesterday by Mr Trump) not top- of- fold headline news everywhere?
Bayer, US, has announced, March 19:
>>Bayer today announced it is joining the U.S. Government’s fight against COVID-19 with a donation of 3 million tablets of the drug Resochin (chloroquine phosphate).
Resochin, a product discovered by Bayer in 1934 and indicated for prevention and treatment of malaria, also appears to have broad spectrum antiviral properties and effects on the body’s immune response. New data from initial preclinical and evolving clinical research conducted in China, while limited, shows potential for the use of Resochin in treating patients with COVID-19 infection.
Bayer in recent days has been in talks with the White House, HHS, CDC, and the FDA, offering any assistance we can provide with a focus on donating Resochin to help in the government’s efforts to combat the virus.
Currently not approved for use in the United States, Bayer is working with appropriate agencies on an Emergency Use Authorization for the drug’s use in the U.S.
Bayer thanks the Trump administration for moving quickly to enable this donation and will continue to work closely with the administration to support its efforts in the fight against COVID-19. >>
Here is Mr Trump’s announcement during what seems to be the now daily Covid-19 White House Covid-19 task force briefing:
No, ABC, it is not merely touting. In recent days, a leading researcher in France has posted a breaking news peer-reviewed report on a clinical test, which has shown remarkable success, which is all over the French language Youtube space, e.g. AP:
Yes, March 4, TWO WEEKS AGO.
The Paper’s Abstract:
>> Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open- label non-randomized clinical trial
Abstract
Background
Chloroquine and hydroxychloroquine have been found to be efficient on SARS-CoV-2, and reported to be efficient in Chinese COV-19 patients. We evaluate the role of hydroxychloroquine on respiratory viral loads.
Patients and methods
French Confirmed COVID-19 patients were included in a single arm protocol from early March to March 16th to receive 600mg of hydroxychloroquine daily and their viral load in nasopharyngeal swabs was tested daily in a hospital setting. Depending on their clinical presentation, azithromycin was added to the treatment. Untreated patients from another center and cases refusing the protocol were included as negative controls. Presence and absence of virus at Day 6-post inclusion was considered the end point.
Results
Six patients were asymptomatic, 22 had upper respiratory tract infection symptoms and eight had lower respiratory tract infection symptoms. Twenty cases were treated in this study and showed a significant reduction of the viral carriage at D6-post inclusion compared to controls, and much lower average carrying duration than reported of untreated patients in the literature. Azithromycin added to hydroxychloroquine was significantly more efficient for virus elimination.
Conclusion
Despite its small sample size our survey shows that hydroxychloroquine treatment is significantly associated with viral load reduction/ disappearance in COVID-19 patients and its effect is reinforced by azithromycin. >>
Going back 15 years, this should not be surprising, as SARS — a closely similar corona virus [some call Covid-19, SARS2], was reported in the virology literature as responsive to Chloroquine:
>>Virology Journal
2, Article number: 69 (2005)
Research Open Access Published: 22 August 2005
Chloroquine is a potent inhibitor of SARS coronavirus infection and spread
Abstract
Background
Severe acute respiratory syndrome (SARS) is caused by a newly discovered coronavirus (SARS-CoV). No effective prophylactic or post-exposure therapy is currently available.
Results
We report, however, that chloroquine has strong antiviral effects on SARS-CoV infection of primate cells. These inhibitory effects are observed when the cells are treated with the drug either before or after exposure to the virus, suggesting both prophylactic and therapeutic advantage. In addition to the well-known functions of chloroquine such as elevations of endosomal pH, the drug appears to interfere with terminal glycosylation of the cellular receptor, angiotensin-converting enzyme 2. This may negatively influence the virus-receptor binding and abrogate the infection, with further ramifications by the elevation of vesicular pH, resulting in the inhibition of infection and spread of SARS CoV at clinically admissible concentrations.
Conclusion
Chloroquine is effective in preventing the spread of SARS CoV in cell culture. Favorable inhibition of virus spread was observed when the cells were either treated with chloroquine prior to or after SARS CoV infection. In addition, the indirect immunofluorescence assay described herein represents a simple and rapid method for screening SARS-CoV antiviral compounds. >>
In short, there has been reason to look seriously at Chloroquine, for fifteen years. That’s why John Delingpole has a point, and a right to ask a pretty pointed question:
>>It ought to be no surprise that chloroquine is effective against both SARS and COVID-19. After all, they are both coronaviruses and COVID-19 has often been described in medical and research sources as SARS-2.
Chloroquine works by enabling the body’s cells better to absorb zinc, which is key in preventing viral RNA transcription – and disrupting the often fatal cytokine storm.
As at least one person has noticed, the implications of this are enormous. If the medical establishment – including CDC – has been aware of the efficacy of chloroquine in treating coronavirus for at least 14 years, why has it not been mass produced and made available sooner?>>
So, should we be focussing significant attention on Chloroquine? Should we be asking pointed questions on how our polarised media may distort our consideration of crucial issues? END
U/D: There is a further report, giving a summary, vid:
Money shot clip of remarks by US Rep Mark Green, a former US Army Flight Surgeon:
The old reliable Malaria drug chloroquine, the newer version hydroxychloroquine has shown really good, three studies, one in Australia, one in China and now one in France mixed with azithromycin, just the old Z-Pac that we take for bronchitis, has had 100%. It cleared the virus, in some cases in three days, that cocktail in every one of the patients in that study . . . It’s very promising, 100% of the virus gone in six days!
Let’s see if this holds up. If so, a breakthrough.
U/D, Mar 22: US vs other per capita Covid-19 death rates (HT, PowerLine):
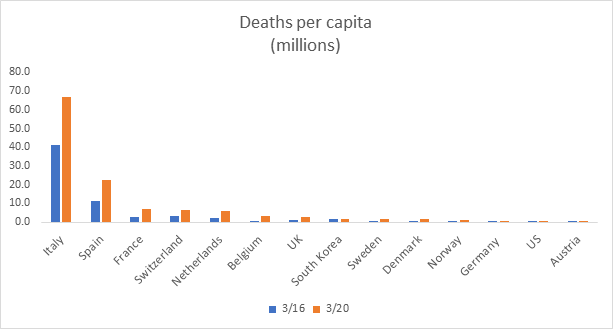
Our friend Brian Sullivan has updated the international mortality table that I posted a few days ago, through yesterday. It shows deaths per million of population in 12 Western European countries, South Korea and the U.S. The blue bar shows the per capita death rate (per million) as of March 16, the orange bar as of March 20 . . . . Italy has the highest mortality rate by far, at 67 per million. It is too early to gauge the ultimate course of the epidemic, but in crude terms it looks as though Italy is heading for a death rate of something like 100 per million. It could easily go higher than that . . . . let’s assume the U.S. ultimately sees a mortality rate of 100 per million. That would be 143 times the current U.S. rate, not outside the realm of possibility. Do the math: if we have around 330 million people, and 100 die per million, that equals 33,000, which would be equivalent to the deaths from an average seasonal flu season. Maybe it’s worse than that; maybe by the time it runs its course, the death toll from COVID-19 rises to 200 per million, 286 times the current rate. That would still be less than the death toll from flu in the U.S. just two years ago.
That gives us some perspective that should help us to turn from over-wrought, deeply polarised rhetoric and political posturing. Then, let us refocus the key point here, there are hopeful potential treatments.
U/D Mar 23: From European CDC, trackers on rate of growth of cases to March 20, in days since hitting 100 cases:
Notice, how China is an outlier on the high side, and Singapore on the low side. Both Canada and the US are in the general European band, Canada happens to lag the US as things got out of containment there later it seems.
U/D Mar 24: As there was a debate overnight on “bell” curve impulses, let us look at the impulse-cumulative effect curve for “serious” cases of Covid-19 for South Korea, which seems to be among the best for statistical records:
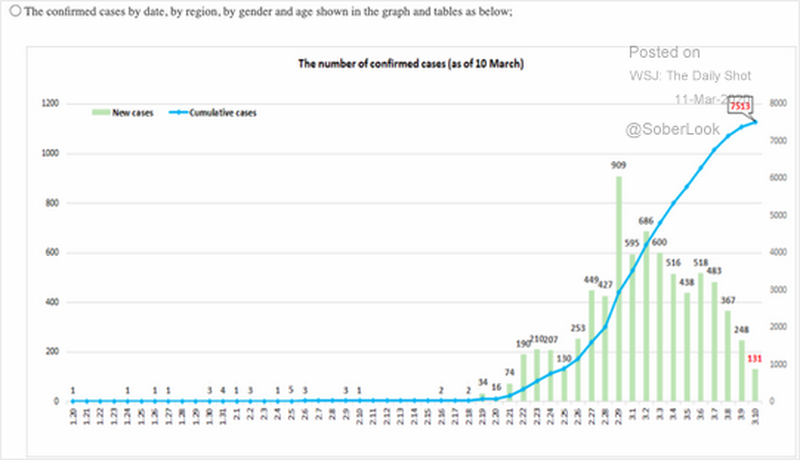
We here see a lin-lin plot [cyan] of the cumulative cases, showing a sigmoid with of course statistical noise. Superposed, to a different scale, is number of fresh cases, shown as a bar chart. The pattern is clear, and is as expected. Notice, the jump in slope at the 909 peak, topping off the concave up part, then the emergence onward of a concave down pattern. The worst day, ironically, marked the point of inflexion where the cumulative case curve began to flatten out.
Next, with that in mind, let us look at the general pattern, using log-lin plots that allow read-off of growth rates etc as we explored yesterday:
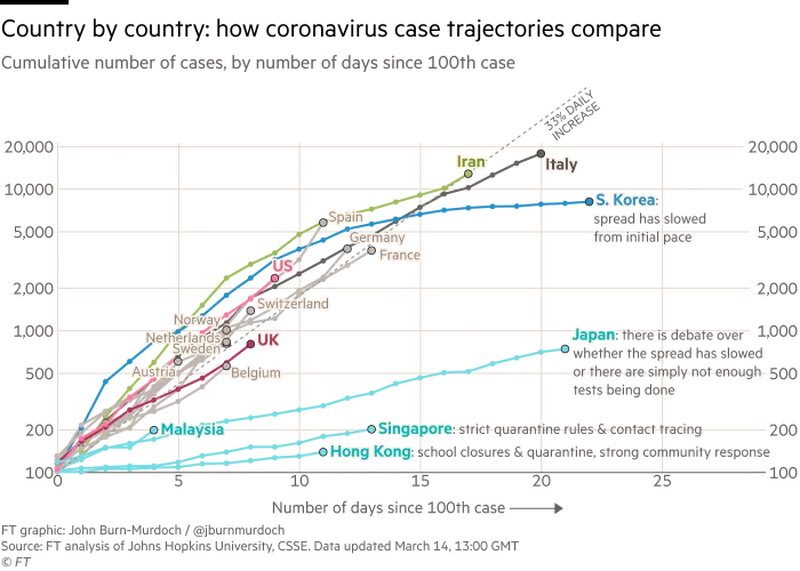
The general sigmoid pattern still appears, obviously, but in a different format. Here, we see that the general pattern once initial lodgement achieves breakout is an early, quasi-exponential growth. In effect, we face an invasion and the first cases form bridgeheads that are prone to breakout, posing a challenge to stabilise by imposing a saturation before the natural one of infecting enough for herd immunity to stop further spread.
Stabilisation is obviously a major challenge.
Notice, too, the “main stream” at doubling every 2 – 3 days that was discussed yesterday. It is notable that the low-rate outliers are asian countries with experience of earlier dangerous epidemics or at least outbreaks, within the past 20 years. That suggests, institutional learning that we may find it advisable to tap. And, it suggests that the policy consensus for Europe and North America is significantly less effective.
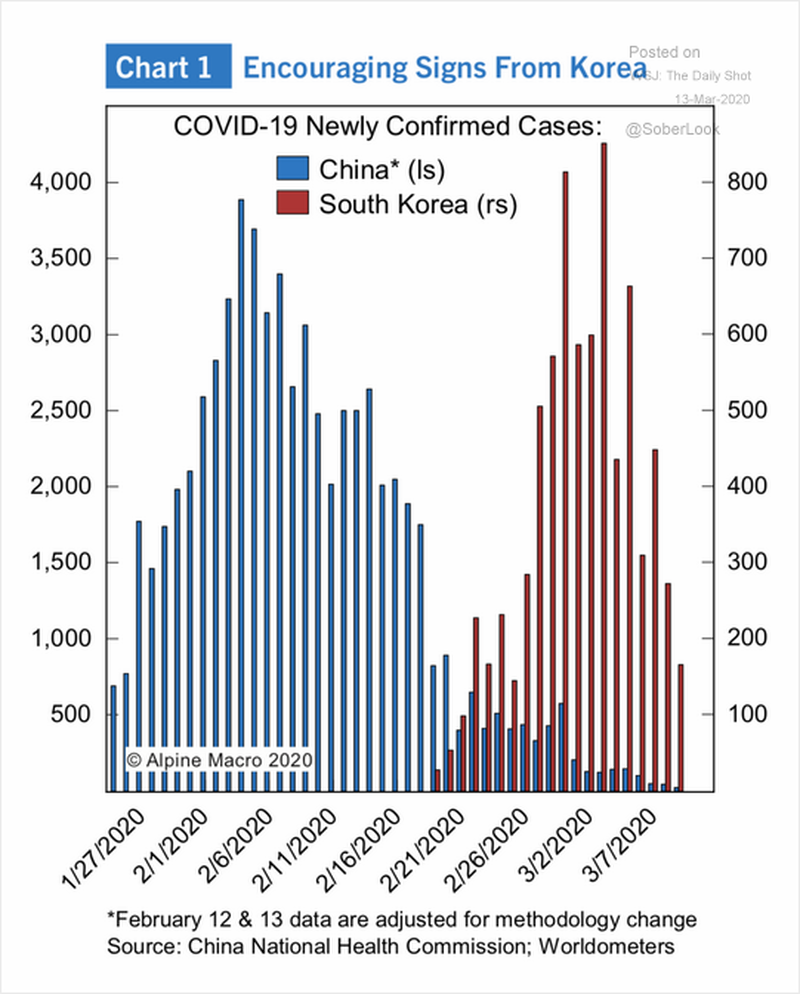
Finally, as a reminder, here are impulse-bells for China and South Korea, overlapped in time: