Jerry drew our attention last night to a radio interview by Dr Vladimir Zelenko. In this interview, he summarises his approach and rationale, giving results and making several announcements. (Unfortunately, the media cannot be embedded at UD as it is not YT. Kindly, go here; and make sure your browser has no active ad blocker.)
On listening last night, here are my first observations on highlight points:
Brazil and Israel are doing his early treatment, clinical diagnosis (backed up by nasal swab test), outpatient-oriented dosage for vulnerable patients protocol, ALT-1. He has treated 405 in that profile and sees 95% reduction on the expected death rate for the n-BAU baseline. He points out that the Raoult [by implication] protocol, which does not use Zn supplements is seeing 90% reduction relative to the same baseline, ALT-2 . . . which is consistent with implications of the tabulated numbers I discussed over the past few days. Several other countries are interested and other physicians are joining in in the US. He intends, with colleagues, to publish in it seems JAMA or NEJM shortly. Long Island has a control group double blind test in train, with results in perhaps 3 – 4 months [implying a smallish test I believe?].
To set context, here, again, is my BAU vs ALT, SWOT-driven, sustainability oriented strategic change decision-making framework:
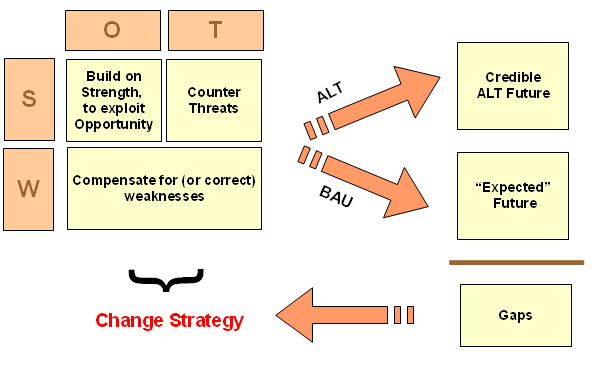
This framework is relevant to the validity of a case based research framework, given that, naturally, there is a [near-] Business As Usual framework. In effect, treat the patients similarly to Flu patients, especially if complications arise. That has yielded a familiar pattern of outcomes for Covid-19, such as we saw in this graphic for China . . . and B & O, summary data with a source are just that, data:
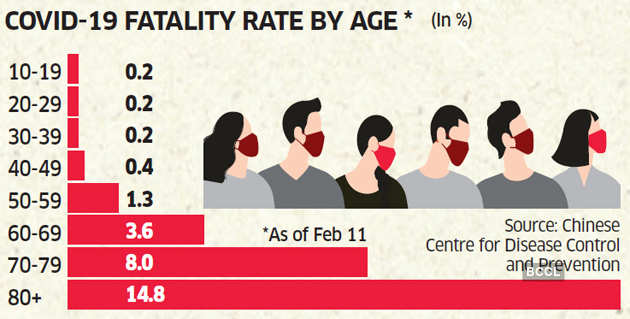
We see here, that age is a critical vulnerability factor. As are several preconditions, especially heart disease.
We therefore have a baseline profile of likely outcomes of Covid-19, a troubling profile. This is n-BAU, with the typical treatments and drugs etc. The pattern of outcomes is as profiled.
In this context, we may now see that Dr Raoult et al [a whole institute in France] and Dr Zelenko et al [it seems, about sixty doctors are using his protocol in a network] are putting on the table two closely related alternatives. Given the suggested mechanism that Hydrochloroquine [HCQ] helps hold open pores that allow Zinc ions to enter the cell at a higher rate than normal, where this is said to help disrupt viral replication, the 5% difference may be significant, and it would be inexpensive to add Zn supplements.
Let us further observe the IHU results as they have moved on since April 18th when we last posted:
This is of course generally compatible with Dr Zelenko’s summary.
These are case study results, which fall afoul of a proposed “Gold Standard” pivoting on double blind, placebo controlled trials. However, they are obviously real observations made in the context of research and treatment in a 3500 bed hospital complex in a major city in France. Indeed, the city that is literally the title for the French national anthem. I can find no good reason to disregard such as no data or not valid tests for ALT-2, especially given the baseline nBAU provided by the hospital.
Where, we may again note, via Google Translate, the approval of protocol:
Research protocol approved by the ANSM [= “Agence Nationale de Sécurité du Médicament et des Produits de Santé (ANSM)”, i.e. National Agency for the Safety of Medicines and Health Products] and the Île-de-France CPP [= “COMITE DE PROTECTION DES PERSONNES ILE DE FRANCE,” i.e. ILE DE FRANCE PERSONAL PROTECTION COMMITTEE] in progress at the IHU Méditerranée Infection: Treatment of respiratory infections with Coronavirus SARS-Cov2 by hydroxychloroquine Acronym: SARS-CoV2quine.”
My follow-up thoughts were:
we have proxies [only] so far, really good numbers are going to require a lot of testing on antibodies and going back through statistical records then calibrating demographically. What we have is tracking the basic dynamics of sigmoids and related models well enough to guide decisions. We are seeing global peaking of wave 1, with China seeing minor onward waves, true Wave 2 is likely, come the next flu season.
Damaging economic and social impacts of the lockdown are leading to early signs, pointing to a need for a managed exit from n-BAU.
With the Raoult-Zelenko protocols allowing early targetted treatment of vulnerable groups on outpatient basis with 90 – 95% reduction in mortality relative to the n-BAU Flu with Complications & ventilators etc baseline, we have a reasonably plausible ALT1 and ALT2 to feed our scenario based planning exercise. The big weaknesses pivot on the polarisation of esp the US and its one-party media, which may cripple and delay moving to ALT-1 until a large wave of needless deaths shifts balance of power.
The use of decision theory and sustainability thinking to counter the threat and compensate for the weakness may help shift balance of power. In particular, the gold standard fallacy must be exposed and corrected. That is, decision theory and BAU vs ALT using the n-BAU protocol as baseline shows an inductively cogent, epistemologiically relevant, ethically responsible answer to required evidence to move forward in the face of polarisation and mischaracterisation.
Selective hyperskepticism has civilisation-level consequences and costs measured in blood and tears through pandemic and needless economic dislocation.
We need to shift back to prudence based responsible rationality.
My projection, currently, therefore is that:
decision theory will prevail over the gold standard evidence threshold fallacy. We will recognise that nBAU gives a baseline comparison with Flu and its treatment so there is no need to give people facing a disease that can kill in 10 days, doing organ damage along the way, sugar pills in order to construct an artificial baseline. We will see evidence being belittled, dismissed and suppressed that points to 90 – 95% reduction in mortality among vulnerable groups for two credible ALTs. We will see that a US$20, outpatient oriented treatment can take pressure off the system, allowing better care for serious cases. We will see that this then allows responsible re-opening of community life and economic activity, leading to a surge in investor and consumer confidence. The lockstep globalist progessivist elites and their media mouthpieces and amplifiers will take a deserved, decisive blow to their credibility and dominance of opinion. As a result, civilisation-level trends are going to shift dramatically, starting with digitalisation of work and education. That’s a Kondratiev, long wave level shift. This pandemic marks a break in history.
Post-pandemic, we are in a different world. END